Basics of Uterine Polyps
Uterine polyps, also commonly known as endometrial polyps are soft fleshy growths attached to the endometrium that is the inner wall of the uterus (or womb) and extend into the uterine cavity. Although uterine polyps have a low incidence rate compared to other reproductive ailments with every one in 10,000 females being affected. However, they can be absolutely worrisome when they straightforwardly affect fertility, pregnancy outcomes, and reoccur after polyp removal. These are somewhat similar to skin tags, which are normal tissues in essence but grow in an abnormal fashion and often flatten out to fit the cavity of the uterus. Endometrial polyps range from a few millimeters in diameter – such as a sesame seed – to several centimeters, like a golf ball or larger. They are attached to the uterine wall by either a large base or a thin stalk (or pedicle). Uterine polyps are commonly observed in 10-25% of women worldwide that are usually in their fifties. These are rare to find in women under 20 years of age or those who have surpassed menopause.
Polyps can occur anywhere in the body ranging from stomach, ear, and nose to different locations in the female reproductive system such as ovarian polyps. It is to be noted that there can be more than one polyp in the uterine cavity. Usually, polyps are contained within the uterus, however, occasionally, they slip down through the cervix (opening of the uterus) and into your vagina, blocking the opening. In such cases, they are referred to as cervical polyps and vaginal polyps, respectively. The vast majority of these polyps are usually noncancerous (benign), although in some cases they can be cancerous or eventually turn into cancer at the end.
Often times people misunderstand the difference between uterine polyps and uterine fibroids since both polyps and fibroids are similar in the essence that they grow on the uterine wall. Statistics show that about 80% of women experience at least one of the conditions in their lifetime. Uterine polyps are oval tissue growths that form in the lining of the uterus; whereas fibroids are benign growths that are found either outside or in the endometrial wall or within the uterine cavity (womb). Fibroids are likely to be developed in younger females, in contrast to polyps that are usually observed in middle-aged women.
Why Do Uterine Polyps Occur?
To date, the exact cause of endometrial polyps in women is not known. However, there are some theories that can best explain why they occur in the first place. These include:
- Hormonal Imbalance: It’s been observed that polyps tend to grow when there is more of the hormone estrogen produced in the body.
- Endometrial hyperplasia: It is the abnormal growth of the uterine lining. Since uterine polyps arise from the endometrial cells which grow during the menstrual cycle in preparation for embryo implantation. In case of absence of pregnancy, this lining sheds; however, due to numerous reasons, if the endometrial lining grows too much, it results in the formation of tissue outgrowth.
- Genetic Factors: Various genetic factors have been found to be linked with the growth of uterine polyps, such as over expression of an enzyme found in the lining of the uterus called aromatase has been found to be one of its causative factors.
Risk Factors for Developing Uterine Polyps
The possible risk factors that increase the chances of developing uterine polyps are jotted down as follows:
- Perimenopause or postmenopausal period
- Hypertension
- Obesity
- Hormone replacement therapy or drug therapy
Uterine Polyps Symptoms
Uterine polyps are rarely symptomatic. However, in case of being symptomatic for these polyps, women show various signs and symptoms such as,
- Irregular menstrual bleeding
- Menorrhagia (heavy menstrual bleeding)
- Bleeding after intercourse
- Cramping in the lower abdomen (dysmenorrhea)
- Infertility or miscarriage
Uterine Polyps Diagnosis and Treatment
After your normal check-up and history, your medical specialist will likely recommend some tests to ensure if the condition correlates to uterine polyps or not. These tests may include vaginal ultrasound, hysteroscopy, endometrial biopsy, and curettage for confirmation.
If you are not symptomatic, then you shouldn’t worry too much about its treatment. However, polyps’ removal becomes a necessity if they are causing any aforementioned symptoms or if they are suspected to be precancerous or cancerous.
Medications: Certain hormonal medications such as drugs that help regulate the hormonal balance, like progestins or gonadotropin-releasing hormone agonists, could be used as a temporary treatment to relieve the symptoms. However, the symptoms will likely return after the medications are stopped.
Surgical removal: Polypectomy is a procedure to remove polyps. The most effective way to perform a polypectomy is through hysteroscopy, in which a small camera is placed inside the uterus using a thin, flexible, lighted telescope (hysteroscope) through your vagina and cervix for visualization of the uterine cavity. The procedure is performed under anesthesia to overcome any discomfort. During the procedure, it is possible to remove polyps from the uterus using a hysteroscope. Curettage is another surgical way to scrape uterine lining and removal of small polyps other than hysteroscopy. Other than that, hysterectomy is performed in cases uterine polyps are found to be cancerous, and thus the whole uterus is removed surgically.
Non-Invasive Solution to Uterine Polyps
Even though surgical removal is one of the available options for the affected females, however, it is not the common and most preferred choice since it involves either cutting you open or putting instruments into your uterus through the vagina. Moreover, the literature suggests that there are about 2.5% – 43.6% chances of recurrence after polypectomy. Additionally, in Asian societies and cultures, like that of Pakistan, fears regarding woman’s loss of ‘virginity’ are insurmountable. Therefore, preserving the virginity of an unmarried female is taken as the utmost priority so that it doesn’t affect their eligibility to get married or their future marital status and life. For this reason, many women remain either undiagnosed or untreated which ends up substantially affecting their quality of life or becomes a threat to their life, in general.
Here is the good news: there is a low-risk and non-invasive alternative procedure to surgical intervention known as 3-D Precision guided uterine artery embolization (UAE), which is now routinely available as an option. This is an outpatient procedure in which the uterine arteries that supply blood to the vascular polyps are located using real-time 3D fluoroscopic equipment. Blood supply to these polyps is blocked by injecting biocompatible particles into the bloodstream through a catheter at the wrist or groin, in which it leads to their ischemic infarction. As a result, they may be dislodged and excrete out from the uterus. This procedure has high success and minimal recurrence rate which eventually restores the quality of life of the affected individuals, taking them back to life.
The facility of 3-D Precision guided uterine artery embolization (UAE), is now available in Pakistan in its two major cities; Karachi and Lahore, by Prof. Dr. Imtiaz Ahmad and his team, who is a renowned interventional radiologist and endovascular surgical specialist with surgical training and extensive experience in Most Advanced Endovascular and Interventional Procedures.


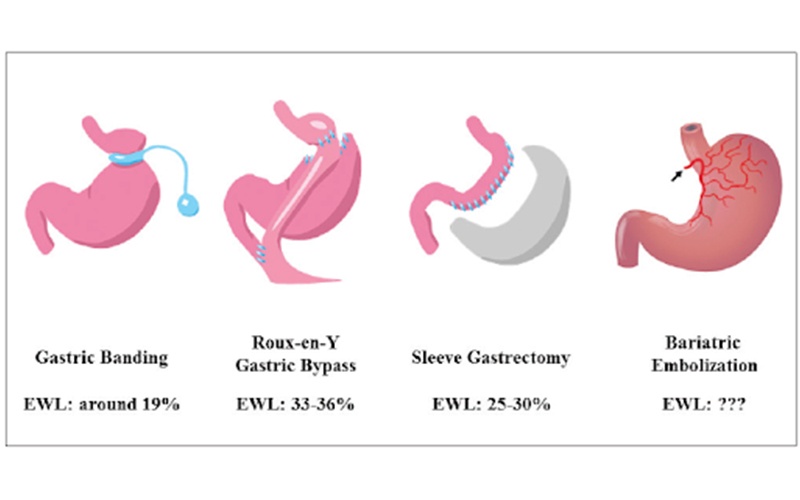 Gastric Banding – In this type of surgical intervention, a ring with an inner inflatable band around the top of your stomach is placed to create a small pouch. The gastric band makes you feel full much sooner after eating a small amount of food.
Gastric Banding – In this type of surgical intervention, a ring with an inner inflatable band around the top of your stomach is placed to create a small pouch. The gastric band makes you feel full much sooner after eating a small amount of food.