OPD Timings
- Farooq Hospital Lahore
Monday – Saturday
(9 am to 8 pm)
Sunday OFF
- Omi Hospital
Monday to Friday
(9 am to 8 pm)
Saturday
(9 am to 8 pm)
Sunday OFF
Contact Info
- Karachi: (021) 32258075 – 79
Lahore: (042) 111 000 043 - Whatsapp: 03312597322
- info@drimtiazahmad.com
For Consultation
Hemorrhoid Embolization
Hemorrhoids are a common anorectal disease that affect millions of people worldwide and are a major medical and socioeconomic problem. Internal hemorrhoids are composed of a dense anastomotic arteriovenous network, the corpus cavernosum recti (CCR). The CCR is dependent on the influx of arterial blood from the branches of the inferior mesenteric artery (the superior rectal arteries [SRAs]). The lower part of the rectum and the anal canal are supplied with blood by the inferior and middle rectal arteries, both of which have origins from the internal iliac artery.
The replacement of muscle tissue with connective tissue causes an expansion of this vascular network of the anorectal submucosa, initiating a negative vicious cycle of progressive vascular dilation and venous insufficiency leading to hemorrhoidal hyperplasia, which in turn causes an increase in arterial inflow in the CCR and leads to symptoms.1-5
Chronic bleeding is the primary symptom of internal hemorrhoids and could be associated with hemorrhoidal prolapse. It is widely accepted that it is difficult for patients to assess bleeding themselves, and assessment is even more difficult in this context, due to the intermittent nature of hemorrhoidal bleeding.
The severity of bleeding symptoms is now assessed according to the bleeding severity score, ranging from 0 (no bleeding) to 9 (daily bleeding with anemia requiring blood transfusions).6 The Goligher classification is used to assess the degree of internal hemorrhoid prolapse from I (no prolapse) to IV (irreducible prolapse).
Following the same principle as DG-HAL, in 2014, we proposed hemorrhoidal artery embolization, termed the emborrhoid technique.11 This technique involves endovascular coil occlusion of the distal branches of the SRA arising from the inferior mesenteric artery. This technique has several advantages: it leaves the hemorrhoidal tissue in place, preserves anal continence, and does not involve the creation of rectal wounds (no local care required).
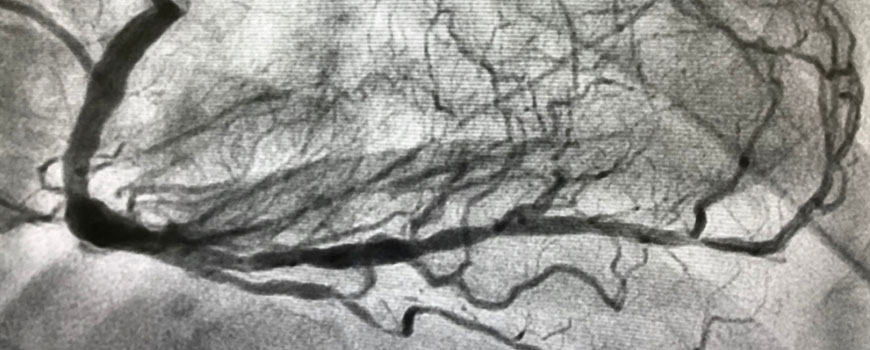
The goal of embolization is not to destroy the CCR, but rather to reduce the blood flow in the CCR. Embolization is performed under local anesthesia via a femoral arterial approach. The inferior mesenteric artery is cannulated with a 4-F Simmons or sidewinder catheter. Angiography is performed to identify all SRA branches supplying the CCR. Each SRA branch is catheterized using a microcatheter. The branches supplying the internal hemorrhoids are embolized with 2- or 3-mm-diameter microcoils. Patients return home on the same day of their treatment.

Technical success is defined as the ability to occlude all target branches from the SRA (Figure 3). If a large anastomotic middle rectal artery is seen on the angiogram, internal iliac artery catheterization is performed to confirm its involvement with the hemorrhoidal vascularization. Embolization of this middle rectal artery is performed with coils. Clinical success is assessed by symptom improvement (reduction in the bleeding severity score and improvement in quality of life) at the 3- and 12-month follow-up visits.
{kind=link}
Results of the emborrhoid technique have been reported by French and European teams.6,11-13 The mean technical success rate is approximately 95%. Catheterization of SRAs is not challenging. The mean number of SRA branches embolized per patient varies from three to six, the mean number of coils used is six (± three), and the mean procedure time is 60 minutes.
At follow-up, the patient satisfaction rate (75%) and quality of life correlate with improvements in the bleeding score (2–3 points). No minor or major complications have been reported based on the Clavien-Dindo and the Society of Interventional Radiology classifications. No cases of anorectal ischemia, anal incontinence, hemorrhoidal thrombosis, or complications related to femoral arterial puncture have occurred.
One-quarter of patients reported that symptoms had not significantly improved enough at 1 year, despite the fact that some underwent a second embolization. Among these patients, some could be considered relative clinical failures with bleeding recurrence under anticoagulation. However, embolization did not decrease bleeding in some patients, likely due to the presence of unrecognized anatomic variations and the effects of coagulation disorders.
Technical failure can occur if the access to the inferior mesenteric artery is not possible (atherosclerosis). In one case, the SRA posterior trunk had a vasospasm during catheterization and embolization of the posterior hemorrhoidal branches could not be achieved.
A limitation of embolization is its possible lack of effect on prolapse (stage IV), which may still require conventional surgical treatment.
Among the nonsurgical minimally invasive techniques available for the treatment of hemorrhoids, RBL offers the best 1-year results with an estimated 50% to 70% success rate.14 DG-HAL is the least invasive surgical technique,15 as it is based on the same physiopathologic concept as embolization and is the most comparable technique to embolization. A recent meta-analysis of 28 studies evaluating DG-HAL showed a pooled clinical success rate of 82.5%.10 A large randomized study comparing DG-HAL and RBL showed a recurrence rate at 1 year of 30% (48/161 patients) and 49% (87/176 patients) for DG-HAL and RBL, respectively.14
There have been no reports of major or minor complications with the emborrhoid technique, which is related to a distal superselective embolization of the SRA hemorrhoidal branches. Preservation of the lower branches feeding the anorectal wall and anastomoses prevents the occurrence of any ischemic complications. The complication rate reported with DG-HAL ranges from 7% to 15%, whereas this is < 5% with RBL.10,14 These complications include pain, bleeding, and urinary retention. Although these complications are generally benign and common for the transanal route, they may prolong the length of hospitalization and delay the return to normal activities.7
Hemorrhoid artery coil embolization is a painless technique that can be performed as an outpatient procedure because there is no direct anorectic trauma. The hemorrhoid technique can also be used in patients who require compassionate care and have surgical contraindications. For these reasons, the emborrhoid technique shows promise for the treatment of hemorrhoids. There is now a clear need for a randomized controlled study, which would confirm the benefits observed with this technique.
- Thompson HF. The nature of hemorrhoids. Br J Surg. 1975;62:542-552
- Schuurman JP, Go PM, Bleys RL. Anatomical branches of the superior rectal artery in the distal rectum. Colorectal Dis. 2009;11:967-971.
- Stelzner F. The corpus cavernosum recti. Dis Colon Rectum. 1964;7:398-399.
- Chung YC, Hou YC, Pan AC. Endoglin (CD105) expression in the development of haemorrhoids. Eur J Clin Invest. 2004;34:107-112.
- Aigner F, Bodner G, Gruber H, et al. The vascular nature of hemorrhoids. J Gastrointest Surg. 2006;10:1044-1050.
- Moussa N, Sielezneff I, Sapoval M, et al. Embolization of the superior rectal arteries for chronic bleeding due to haemorrhoidal disease. Colorectal Dis. 2017;19:194-199.
- Simillis C, Thoukididou SN, Slesser AA, et al. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102:1603-1618.
- Watson AJ, Hudson J, Wood J, et al. Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): a pragmatic, multicentre, randomised controlled trial. Lancet. 2016;388:2375-2385.
- Aigner F, Bodner G, Conrad F, et al. The superior rectal artery and its branching pattern with regard to its clinical influence on ligation techniques for internal hemorrhoids. Am J Surg. 2004;187:102-108.
- Pucher PH, Sodergren MH, Lord AC, et al. Clinical outcome following Doppler-guided haemorrhoidal artery ligation: a systematic review. Colorectal Dis. 2013;15:e284-294.
- Vidal V, Louis G, Bartoli JM, Sielezneff Y. Embolization of the hemorrhoidal arteries (the emborrhoid technique): a new concept and challenge for interventional radiology. Diagn Interv Imaging. 2014;95:307-315.
- Vidal V, Sapoval M, Sielezneff Y et al. Emborrhoid: a new concept for the treatment of hemorrhoids with arterial embolization: the first 14 cases. Cardiovasc Intervent Radiol. 2015;38:72-78.
- Zakharchenko A, Kaitoukov Y, Vinnik Y, et al. Safety and efficacy of superior rectal artery embolization with particles and metallic coils for the treatment of hemorrhoids (Emborrhoid technique). Diagn Interv Imaging. 2016;97:1079-1084.
- Brown SR, Tiernan JP, Watson AJM, et al. Haemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second-degree and third-degree haemorrhoids (HubBLe): a multicentre, open-label, randomised controlled trial. Lancet. 2016;388:356-364.
- Zagryadskiy E, Gorelov S. Transanal Doppler-guided hemorrhoidal artery ligation and recto anal repair vs closed hemorrhoidectomy for treatment of grade III-IV hemorrhoids. A randomized trial. Pelviperineology. 2011;30:107-112.
Dr. Ahmad has been practicing in the health care industry for more than 20 years.
In 1995 he completed his fellowship at Northwestern University Chicago Illinois USA.